
If you live in a rural area, getting healthcare can feel like a full-time job. The nearest doctor might be an hour away, and when you finally get there, appointments are booked for months. Add in high costs, long drives, and limited options, and it’s easy to see why so many people delay care until it’s urgent.
Across rural America, millions of people face these same challenges every day. From transportation barriers to provider shortages and spotty internet that limits telehealth, rural communities are caught in a cycle that makes staying healthy harder than it should be.
In this post, we’ll break down the biggest barriers to healthcare in rural areas and explore real-world solutions that are already making a difference.
How Geographic Isolation Creates a Perfect Storm of Healthcare Challenges
Geographic isolation doesn’t just mean longer drives to medical appointments. It creates interconnected problems that feed on one another, making rural healthcare access increasingly difficult. When rural hospitals close, they don’t just eliminate emergency services. They trigger a domino effect in which primary care doctors leave, pharmacies shut down, and ambulance services are stretched beyond capacity.
Distance compounds every other barrier. A 90-mile round trip to see a specialist isn’t just about transportation costs. You’re looking at lost wages, childcare arrangements, and the physical strain of travel when you’re already sick. Many rural residents delay care until conditions become emergencies, which drives up costs and worsens outcomes.
What makes this particularly challenging is how these barriers reinforce each other. Poor internet connectivity limits telehealth options. Sparse populations make it harder to justify keeping services local. The result is a self-reinforcing cycle that leaves rural communities increasingly isolated from quality healthcare.
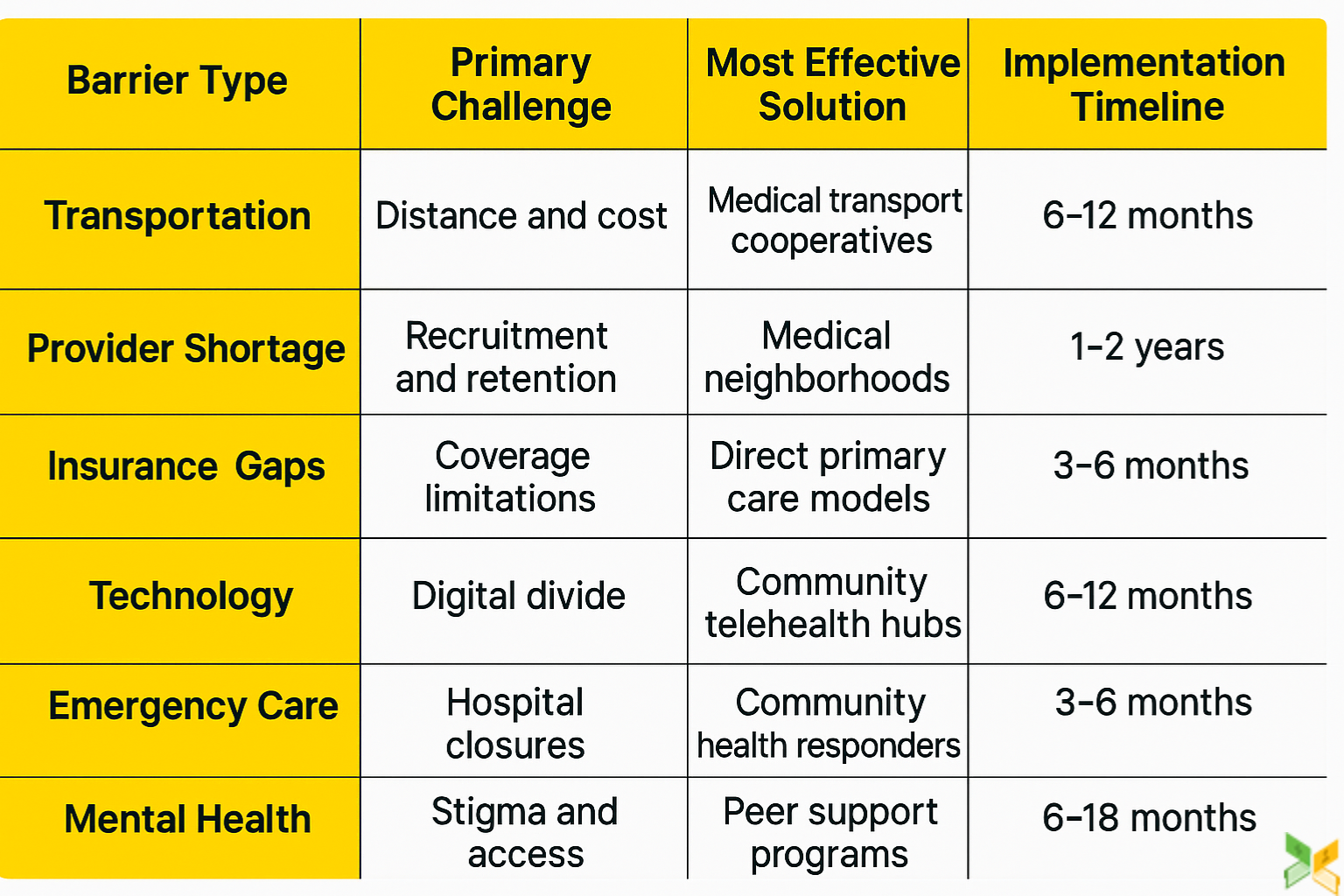
Key Barriers to Healthcare Access in Rural Areas
Rural communities face unique healthcare challenges that urban residents rarely encounter. These barriers to healthcare in rural areas create complex problems requiring targeted solutions. Let’s examine the specific obstacles that make healthcare harder to access in rural communities.
Transportation Deserts: When Getting There is Half the Battle
Getting to healthcare appointments becomes a major undertaking in rural areas. Rural residents travel an average of 40 miles one-way for specialty care, but distance is just part of the problem. The hidden costs add up fast between gas, potential overnight stays, and lost wages from time off work.
Interestingly, access to primary healthcare is generally well distributed, with >90% of the rural population living within 15 minutes of a basic healthcare facility. However, that remaining 10% often faces significant challenges, especially in extremely remote areas.
Some communities are finding creative solutions. An example lies in the actions of the government of Castilla-La Mancha, which created a demand-responsive health transport service benefiting 15 municipalities and 18,200 inhabitants, with 3 minibuses, 14 taxis, and a digital application for booking journeys. These grassroots transportation cooperatives are proving more sustainable than waiting for government programs.
The Provider Shortage Spiral: Why Doctors Don’t Stay
The rural physician shortage isn’t just about recruiting new doctors. It’s about keeping them. Rural doctors report burnout rates 20% higher than urban colleagues, primarily due to being on call more frequently and handling broader conditions without specialist backup.
Rural areas are especially vulnerable to shortages and limited resources, forcing several to reduce or even close services. This is detrimental to communities in need of essential services, particularly when considering that roughly 75 million people live in a primary care Health Professional Shortage Area (HPSA).
The most successful retention programs aren’t just offering loan forgiveness. They’re creating “medical neighborhoods” where providers share call duties across multiple small hospitals, reducing individual burden while maintaining coverage. This collaborative approach helps combat the isolation that drives many rural physicians away.
Insurance Gaps: When Coverage Doesn’t Cover Enough
Having insurance doesn’t guarantee affordable healthcare in rural areas. Rural insurance markets often have limited plan options, with deductibles averaging $3,000 higher than urban plans. Many rural residents face the “coverage cliff,” earning just enough to disqualify for subsidies but not enough for comprehensive coverage.
Limited access to healthcare becomes a financial issue even with insurance. Local specialty providers often reject Medicaid and federal assistance programs, making it difficult for patients to obtain the advanced care they need. This forces referrals to distant tertiary care centers that charge much higher rates.
Some rural hospitals are pioneering “direct primary care” models where patients pay monthly fees for unlimited primary care access, bypassing insurance entirely for basic services. These innovative approaches help address the lack of access to healthcare by making routine care more affordable and predictable.
Technology Barriers: The Digital Divide in Healthcare
While telehealth sounds like the perfect rural healthcare solution, reality is more complex. Twenty-five percent of rural households lack broadband access, and many more have connections too slow for video consultations. This digital divide means communities that could benefit most from telehealth often can’t access it.
Some areas are creating “telehealth hubs” at libraries, community centers, and grocery stores. These locations provide high-speed internet and private spaces for virtual medical appointments. This approach helps bridge the technology gap while maintaining patient privacy.
The challenge of what can limit access to health care services extends beyond just internet speed. Many rural residents lack the digital literacy or devices needed for telehealth appointments, creating additional barriers to this promising solution.
Specialist Shortage: The Referral Roadblock
Rural areas have 30% fewer specialists per capita than urban areas, but coordination of care creates even bigger problems. Rural primary care doctors often struggle to get timely specialist consultations, leading to delayed diagnoses and treatment.
“Hub and spoke” telemedicine programs are emerging where urban specialists provide regular virtual consultation hours specifically for rural providers. This allows same-day specialist input on complex cases, dramatically reducing wait times and improving patient outcomes.
These collaborative models help address the fundamental issue of specialist scarcity while maintaining the doctor-patient relationship with local primary care providers. They represent a sustainable approach to expanding specialty access without requiring full-time specialists in every rural community.
Emergency Care Gaps: When Minutes Matter
Since 2010, 136 rural hospitals have closed their emergency departments, leaving some communities 50+ miles from the nearest emergency care. This creates “EMS deserts” where ambulance transport times exceed the critical “golden hour” for stroke and heart attack treatment.
Rural communities are responding by training volunteer “community health responders.” These locals receive basic medical training to provide immediate care and assist with coordinating emergency transport. While they can’t replace full emergency departments, they fill critical gaps in the response chain.
The loss of local emergency care forces rural residents to make difficult decisions about when to seek help. Many delay calling for assistance, hoping conditions will improve, which often leads to worse outcomes when treatment finally occurs.
Mental Health Stigma and Access: The Hidden Crisis
Rural areas have suicide rates 46% increased than urban areas, partly due to provider shortages but also because of cultural stigma around seeking mental health care. Traditional therapy models often don’t work in small communities where everyone knows everyone.
Peer support models are proving highly effective in rural areas. Training community members to provide mental health first aid and ongoing support reduces stigma while building local capacity. These programs work because they respect rural values of neighbor helping neighbor.
The lack of access to healthcare in rural areas becomes particularly acute for mental health services. Rural residents often drive hours to see specialists, making regular therapy sessions impractical and expensive.
Pharmacy Deserts: The Medication Access Challenge
Independent pharmacies are closing in rural areas at twice the rate of urban pharmacies, creating “pharmacy deserts” where residents drive 30+ miles to fill prescriptions. This particularly impacts seniors who may need multiple medications regularly.
Some rural areas are piloting “pharmacy-in-a-box” programs where automated dispensing units in community centers provide common medications with remote pharmacist oversight. These innovative solutions help maintain local access while reducing overhead costs.
Mail-order pharmacy options and 90-day prescription fills can help reduce trips for medication refills. However, these solutions don’t address the loss of local pharmacist expertise and medication counseling that independent pharmacies traditionally provided.
Maternal and Child Health Gaps: Starting Behind
Over half of rural counties lack hospital-based obstetric services, forcing pregnant women to travel hours for delivery. This contributes to rural maternal mortality rates that are higher than urban rates.
Rural birth centers staffed by certified nurse-midwives are showing excellent outcomes for low-risk pregnancies while keeping care local. These facilities can handle more births and maintain transfer agreements for high-risk cases.
Early prenatal care becomes especially important in rural areas where emergency obstetric services may be distant. However, accessing this care can be challenging due to provider shortages and transportation barriers.
Chronic Disease Management: The Self-Care Challenge
Rural residents have higher rates of diabetes, heart disease, and obesity, but fewer resources for ongoing disease management. Limited access to nutritionists, diabetes educators, and cardiac rehabilitation programs makes self-management more difficult.
Community health worker programs are proving highly effective in rural areas. Training residents to provide ongoing support and education for chronic disease management creates sustainable, culturally appropriate care models.
These peer-led programs work because they understand local contexts and barriers. Community health workers can address transportation issues, insurance questions, and medication access in ways that distant specialists cannot.
Taking Action on Rural Healthcare Access
Breaking down barriers to healthcare in rural areas requires understanding that these challenges are interconnected. Solving transportation issues won’t help if there aren’t providers to see, and recruiting providers won’t work if communities can’t sustain them financially.
The most promising solutions combine innovation with community engagement, from telehealth hubs in libraries to peer support networks that build on rural values. Success comes from thoughtfully combining high-tech solutions with community-based care that respects rural strengths while addressing specific challenges.
FAQs on Rural Healthcare Barriers
1. How do transportation costs affect rural healthcare access?
Transportation costs often exceed the actual medical visit cost, forcing patients to delay or skip necessary care entirely.
2. Can telehealth really replace in-person visits?
Telehealth works well for follow-ups and consultations, but can’t replace all in-person care, especially procedures and physical exams.
3. What can limit access to health care services?
Access to healthcare is often limited by financial constraints, provider shortages, transportation issues, and long wait times. Additional barriers include language and cultural gaps, lack of insurance, and personal challenges like work commitments or fear of seeking care.