
You’re trying to hit value-based care targets with scattered data across EHRs, claims, labs, and patient sources. Meanwhile, your patients don’t fit tidy clinical trial criteria, and leadership wants proof programs work now, not later. Healthcare Real World Data (RWD) provides comprehensive insight into how treatments perform in everyday clinical settings, not just controlled trials. RWD becomes the difference between guessing and managing, transforming value-based healthcare from a contract model into an operating model.
Real World Data is The “Missing Scoreboard” Value-Based Care Can’t Run Without
Value-based healthcare only works when you can measure outcomes that matter to patients and connect them to cost across the full care journey. Without RWD, you can’t see whether care pathways actually improve patient health or just add more activity.
RWD fills gaps that claims-only approaches leave behind. It helps track longitudinal outcomes, uncover hidden cost drivers like medication non-adherence, and identify which interventions move the needle for specific populations. Most importantly, RWD turns value-based care into an operating model where teams learn, adjust, and prove impact continuously.
Track Outcomes People Actually Feel, Not Just What’s Easy to Bill
Patient-reported outcomes are not optional metrics. They often serve as the earliest signal that care plans are failing, well before utilization patterns appear in claims data. When combined with social determinants of health data, these insights become even more powerful. SDOH factors such as transportation access, food security, housing stability, and caregiver support frequently explain why patients struggle to follow prescribed care plans.
Many organizations reference patient-reported outcome measures, but few explain how they connect to value-based care measurement loops. Integrating patient-reported outcomes with SDOH data creates a clearer view of risk, adherence barriers, and intervention timing.
Start by embedding lightweight patient-reported outcome workflows into one high-volume pathway using existing patient portal surveys or SMS check-ins. Layer in SDOH screening questions where appropriate to identify social risk drivers early. Review responses weekly in team huddles to flag failing care plans before they escalate into costly complications.
Validated tools such as EQ-5D, PHQ-9, and PROMIS integrate effectively with EHR patient portals and SMS survey platforms, allowing both clinical symptoms and social risk factors to be monitored in the same feedback loop.
Find Real Cost Drivers Hiding Between Visits
RWD becomes most powerful when it links clinical severity, social risk, and utilization together. Otherwise, you misread “high cost” as “high need” and fund the wrong programs.
Build a “top 50 rising-risk” list combining recent ED visits, medication gaps, and missed appointments. Route these patients to care management within 48 hours. Risk stratification using claims plus EHR data, along with social determinants screening tools, reveals patterns you’ll miss looking at billing data alone.
Spot Which Care Pathways Work in The Real World, Not Just On Paper
Understanding performance on paper is only part of the equation. The real insight comes from examining how care pathways function under real-world conditions. The visual below highlights where breakdowns typically occur and how to identify them.
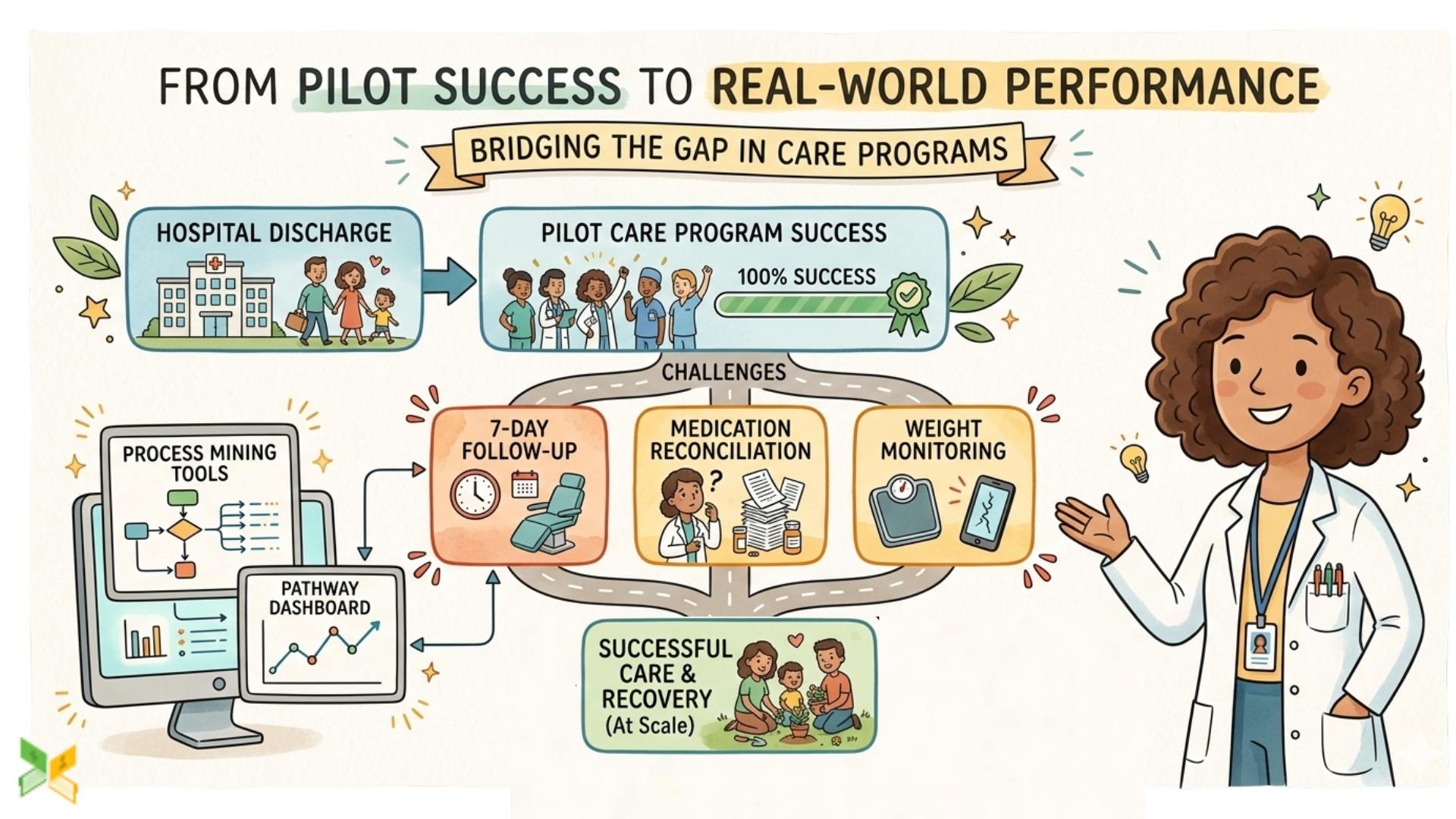
Once leakage points are clearly identified, the focus shifts from observation to correction. Addressing workflow friction and access barriers at these specific stages strengthens outcomes, improves adherence, and reduces avoidable costs across the system.
Reduce Readmissions by Predicting Risk Earlier
By analyzing patterns in their EHRs, hospitals can identify patients likely to benefit from extra support, resulting in reduced emergency room visits and boosted patient satisfaction. Predictive models trained on incomplete labels miss early warning opportunities when you add patient-generated and nursing notes data.
Start with rules-based “early warning” layers before machine learning. Recent discharge, abnormal labs, plus missed follow-up create actionable alerts. The LACE index provides a solid baseline before adding more complex modeling. Validate weekly with clinicians to build trust in your risk predictions.
Make Quality Measurement Fair by Adjusting for Case Mix
Value-based care metrics can punish providers serving complex populations unless RWD adjusts for risk and enables equity-aware benchmarking. Standard quality measures often miss the complexity of real patient populations.
Segment outcomes by race, ethnicity, ZIP code, language, and comorbidity burden. Review gaps as standing quality improvement agenda items. CMS risk adjustment concepts and social determinants variables help create fair comparisons between different provider populations.
Turn RWD Into Action With Closed-Loop Workflows
Dashboards don’t change outcomes – workflows do. The missing piece is turning insights into tasks, assignments, and follow-up confirmation.
For one metric like uncontrolled A1c, create automated work queues: outreach leads to appointment, medication review, then recheck lab. Care management platforms with EHR tasking and rules engines turn data into coordinated action rather than just reports.
Understanding how RWD transforms daily operations sets the stage for practical implementation across your organization.
Implementation Game Plan: How to Start Using RWD in Value-Based Healthcare
Pick One High-Impact Use Case And Lock The Definition of Success
Accountable care organizations provide excellent examples by pooling clinical data from multiple providers to assess which interventions have the greatest impact on patient populations, leading to better care and lower costs. Most RWD programs fail because teams start with “healthcare data” instead of the decisions they’re trying to improve.
Choose one focus: readmissions, total cost of care, diabetes control, or episode costs. Define success metrics and assign owners before touching any data. Create a one-page use case charter with clear outcomes that everyone understands.
Build Governance That Moves Fast And Survives Audits
Governance isn’t red tape when done right – it makes evidence defensible to payers and regulators. In value-based care, governance determines whether your insights can actually influence contracts and quality scores.
Create a small RWD council with clinical, data, privacy, and operations representatives. Meet weekly for 30-minute decision sessions with clear change logs. Data provenance checklists and access control matrices turn governance from a barrier into a competitive advantage.
Choose Architecture For Value-Based Care Partnerships
Architecture should match your partnership reality. Networks often need hybrid models balancing local control with shared analytics capabilities.
If you share data across entities, pilot federated analytics that keep data local while enabling collaborative insights. For mostly internal use, build curated outcomes marts first. Trusted research environments and tokenization help maintain privacy while enabling the data linkage value-based care requires.
Validate Insights With Clinicians Before Automating
Statistical significance doesn’t equal clinical sense. Value-based care wins require clinician trust in the measures and triggers you’re using to manage populations.
Run “chart review rounds” on 20 cases behind each signal, like predicted readmission. Refine variables based on clinical feedback. Model cards and explainability summaries help clinicians understand and improve your risk prediction logic.
Even solid implementation plans can stumble on common mistakes that undermine real-world data projects.
What Competitors Get Wrong About RWD in Value-Based Care
Treating RWD Like an IT Project Instead of a Care Delivery Capability
The strongest value-based care organizations use RWD to run weekly improvement cycles, treating it like operations rather than research. Many competitors implement technology without changing how care teams actually work.
Add one RWD-driven metric review into the existing operational rhythm. Weekly service line meetings with task triggers turn insights into care improvements. Quality improvement cycles and operational dashboards create sustainable change rather than one-time reports.
Using Privacy as an Excuse Instead of a Competitive Advantage
Healthcare systems face growing complexity in determining where data privacy might be compromised, with different departments prone to varying risk levels, making consistent security approaches difficult. Smart organizations turn privacy requirements into collaboration opportunities through secure computation and federated approaches.
Implement privacy-preserving analytics that let you collaborate without risking patient trust. Bring-algorithm-to-data approaches, and trusted research environments enable insights without centralizing sensitive information. Privacy-by-design becomes a competitive advantage in partnerships.
Moving beyond common pitfalls brings up practical questions about implementing real-world data strategies.
Moving Healthcare Forward with Real-World Data
Healthcare Real-World Data transforms value-based care from theory into practice by connecting patient outcomes to costs across complete care journeys. The future healthcare system makes decisions backed by real-world data, not just theories. Organizations implementing RWD strategies now will lead tomorrow’s value-based care landscape, while others struggle with outdated measurement approaches.
Common Questions About Healthcare Real-World Data In Value-Based Care
1. What’s the biggest challenge using real-world data in value-based healthcare?
Misaligned definitions between teams measuring the same metrics differently, plus incomplete longitudinal records when patients receive care outside your system.
2. Is real-world data reliable enough for value-based care decisions?
Yes, when you triangulate sources and test for bias. EHR plus claims plus patient-reported outcomes creates reliability sufficient for care improvement and resource allocation decisions.
3. How can providers start using real-world data in value-based programs?
Start where care teams feel pain: readmissions or chronic disease management. Build a minimum viable dataset with one pilot dashboard tied to workflows, not just reports.